

The margin problem in healthcare IT consulting
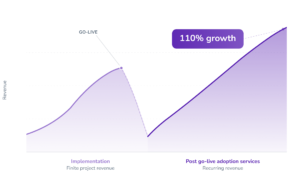
Healthcare IT consulting has a revenue model with a built-in expiration date. You staff up for a go-live, deploy for 12 to 24 months, hit the switch, and move on. Every successful implementation is a revenue stream ending.
The interesting number is what happens next. KLAS Research reports that EHR clinical optimization engagements grew more than 110% from 2018 to 2024, based on validated project data. That growth did not come from new implementations. It came from provider organizations discovering that go-live was not the finish line.
If you run a healthcare IT consultancy, the strategic question is no longer which go-live comes next. It is whether you own what happens after.
The post go-live gap
Implementation teams leave. Clinical systems are live. And adoption stalls. The pattern is remarkably consistent.
KLAS’s Arch Collaborative data puts the scale in sharp terms: just 38% of organizations say their recent EHR implementation hit the mark. Satisfaction with implementations has dropped consistently since 2022, declining more than twice as much as any other metric in KLAS’s standard evaluation. The clinical experience data reinforces the pattern: KLAS burnout scorecards show 67% of physicians and 45% of nurses do not feel their EHR helps them work efficiently. Among burned-out physicians, 62% cite the EHR as a major contributor.
This is not a training gap. Training happened before go-live. This is an adoption gap: the distance between a system being available and a system being used well. And it persists because the traditional post go-live toolkit was designed for the first weeks, not the first year:
- Floorwalkers for the stabilization period, then gone
- Tip sheets and quick-reference cards that go unread within a month
- Classroom refresher sessions that pull clinicians off the floor
- Help desk tickets as a proxy for learning, with no feedback loop to fix the root cause
Every one of those methods ends or degrades. None of them produce a measurable, recurring service line.
Where the recurring revenue sits
Four service lines are emerging for consultancies that want to stay in the relationship after go-live. Each can be structured as an ongoing engagement rather than a one-time project.
Optimization analytics
The most evidence-backed service line. The University of Colorado’s Sprint program, published in Mayo Clinic Proceedings and JAMIA Open, demonstrated that structured optimization sprints shifted clinician satisfaction from −15 to +12 on a −100 to +100 scale. Burnout endorsement dropped from 39% to 34%. The financial case is equally concrete: a NorthShore University HealthSystem study in Applied Clinical Informatics found that an 11-member optimization team costs roughly $1.2 million annually and saves approximately $2.5 million in physician turnover and burnout replacement costs. The authors’ conclusion: the program pays for itself.
Adoption measurement
What gets measured changes. The question is what you measure. This is where frameworks like HEART (Happiness, Engagement, Adoption, Retention, Task success) earn their place: they give consultancies a structured, repeatable way to quantify adoption across applications and sites, turning subjective impressions into scorecards that clients can act on. Not login counts. Not training completion percentages. Five dimensions that map to the operational outcomes a CIO actually cares about.
Ongoing contextual support
The shift from classroom training to in-workflow assistance is not a technology trend. It is a staffing reality. A CHIME-member survey conducted by CereCore found that 81% of CIOs hire contractors for specific short-term projects, and over half have contracted for partial IT outsourcing. Stoltenberg’s annual Health IT survey identified retaining and budgeting for qualified IT resources as the top operational challenge for the fourth straight year. Provider organizations cannot staff their way out of the adoption gap. Consultancies that can deliver contextual, in-application support as a managed service fill a gap their clients cannot close internally.
AI adoption governance
AI tools are arriving faster than clinical teams can absorb them. Dragon Copilot, DAX Copilot, Abridge, and general-purpose assistants like ChatGPT and Copilot are entering clinical and administrative workflows. The consulting opportunity is threefold: measure which teams actually use sanctioned AI tools, identify where unsanctioned alternatives create compliance risk, and provide structured adoption support as new AI capabilities roll out. If you already run post go-live adoption services, AI governance is not a new sale. It is a scope expansion your clients are already asking for.
Why the economics are shifting
Three forces are pushing healthcare IT consulting from project-based toward recurring models.
Black Book Market Research reports that IT managed services in healthcare account for $60 billion, with 59% of hospitals with over 150 beds moving toward more outsourcing. Deloitte’s 2026 Global Health Care Outlook, surveying 180 health-system executives, found workforce remains the number-one concern, with Deloitte recommending investment in workforce engagement, digital and AI tools, and partnership models that improve operating margins. And the capital markets agree: recent acquisitions (Tegria by Altaris, Nordic by Accrete Health Partners) signal that investors see recurring-revenue healthcare IT services as the thesis, not project-based staffing.
Becker’s Hospital Review frames the shift well, calling EHR optimization “the new EHR lifecycle” and noting that optimizations work best when started one to two months post go-live, because organizations simply cannot fit everything into an implementation. The firms winning these engagements are building recurring practices anchored on analytics, measurement, and managed support.
What these service lines require
Delivering post go-live services at scale requires two capabilities that most consultancies do not yet have.
Application Intelligence: the ability to see how clinical teams actually use software and AI tools across applications, sites, and roles. Usage patterns, feature adoption, friction points, and performance differences between high-performing and struggling sites, quantified and comparable. Without this visibility, optimization is guesswork.
Contextual Assistance: help delivered inside the application at the moment of need, not in a classroom six weeks before go-live. In-workflow guidance, contextual support, and change communication that reaches clinicians without pulling them out of their work.
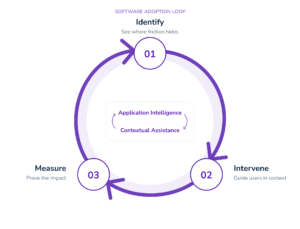
The combination is what makes a recurring practice viable:
- Application Intelligence identifies where adoption is falling short
- Contextual Assistance delivers the intervention
- Application Intelligence measures the result
That closed loop is both the proof that justifies ongoing engagement and the diagnostic that surfaces the next opportunity. Consultancies that can run it hold a service line their clients will renew year after year.
The firms building this now will own what comes next
EHR implementations are not going away. But here is the question worth sitting with: if optimization engagements grew 110% in six years while implementation satisfaction dropped to 38%, where is the growth in healthcare IT consulting over the next decade?
The consultancies that build a structured practice around optimization analytics, adoption measurement, contextual support, and AI governance will not be waiting for the next go-live to fill their pipeline. They will already be inside the account, running the adoption scorecard, proving the outcomes, and having the renewal conversation before the client raises it.